
Trigger Point Pain For Pectoralis Major Muscle
Pectoralis Major Trigger Point
The pectoralis major has two origins. One is in the clavicular head at the anterior border of the medial half of the clavicle. The other is in the sternocostal head, at the anterior surface of the sternum, the superior six costal cartilages, and the aponeurosis of the external oblique muscle: Clavicular head: C5 and C6; and Sternocostal head: C7, C8 and T1. The insertion is found at the lateral lip of the bicipital groove of the humerus (anteromedial proximal humerus), while the nerves that serve the pectoralis major are the lateral pectoral nerve and medial pectoral nerve.
The trigger point causes referral pain in the torso, which leads to primary pain symptoms in the front of chest, front of shoulder, medial epicondylar, and also hypersensitive nipples and/or breast. These pain symptoms can also develop into rapid or irregular heartbeat, which causes heart attack-like pain, volar wrist & palmar pain. Secondary symptoms can develop dorsal finger pain and ulnar forearm pain.
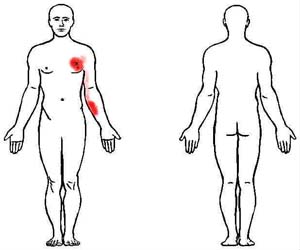
The trigger point in the picture below shows how the main areas of pain (shown in dark red) begin in the chest and arm, with the path moving down the inner arm.
Pectoralis major muscles becomes hyperactive and in spasm with chronic slouching postures. The head and shoulders rounding forward cause the pectoralis major to tighten and limit shoulder flexibility. Over time the shoulders roll inward and shoulder flexibility decreases. Trigger points eventually develop in the muscles causing radiating arm pain past the elbow.
Chronically shortened pectoralis major muscles contribute to neck and shoulder pain by changing the normal mechanics and postures. The altered positions of the shoulder increase stress and strain on the muscles leading to sprains, strains, and tendinosis.
Conservative Treatments
Therapeutic treatments for addressing soft tissue injuries involve massage therapy, manual therapy, trigger point therapy, Graston Technique, or Active Release Technique. These treatments increase blood flow, decrease muscle spasms, enhance flexibility, speed healing, and promote proper tissue repair.
When these treatments are incorporated into a treatment plan patients heal faster and are less likely to have long-term pain or soft tissue fibrosis or scar tissue in the injured muscle. These soft tissue treatments are incorporated with therapeutic exercise and flexibility programs
Treatment for shoulder injuries often requires a variety of exercises, stretches, conservative treatments, medical treatments, and home therapies. Shoulder injuries can become chronic if the appropriate steps are not taken.
Elbow injuries often occur in people with severe or chronic shoulder injuries. People begin trying to alter their shoulder motions to protect it. Unfortunately these altered body mechanics tend to overwhelm the muscles and tendons around the elbow. People often develop a secondary cubital tunnel syndrome, lateral epicondylitis, tricep tendonitis, medial epicondylitis, pronator teres syndrome, double crush, carpal sprains, wrist tendinitis, de quervain's tendonitis, finger extensor strains, or carpal tunnel syndrome.
Treatment for elbow injuries can be extensive if the tendinosis is severe. Mild strains can be treated at home with PRICE, home stretches, and exercises. Don’t wait for damage to both the shoulder and elbow to seek treatment and therapy.
Medical Treatments
NSAIDs are often prescribed for the initial acute injury stages. In severe cases that involve multiple joint regions, muscle relaxers or oral steroids can be given. Trigger point injections, botox, or steroid injections can be treatment options. Pain management is not usually required unless stronger medications or joint injections are required for treatment.
MRI and X-rays will not usually be ordered to evaluate mild to moderate muscle, tendon, and ligament injuries. Severe cases may utilize advanced imaging to rule out bone fractures, edema, nerve entrapments, tendon or muscle ruptures. NCV testing may be utilized in cases that also involve muscle, sensory, or reflex loss.
Cervical spinal disc bulges and herniations onto the spinal cord or nerve root produce different symptoms and location of symptoms. Pain radiating in the hand is one symptom; along with numbness, weakness, fatigue, loss of sensation, or reduced reflexes. Your chiropractor, physical therapist, occupational therapist, or physician will evaluate your condition and make a proper diagnosis and treatment recommendations. Ask them any questions you might have about your injury.
Many people do have arthritis or degenerative changes in their elbow, wrist, finger, or thumb joints. Arthritis does not mean you will always have pain in the joints. Degenerative arthritis means the structural Integrity of the bones have changed which alters its gliding, sliding, and hinging motions. The more severe the arthritic changes the easier it becomes to aggravate the joint and produce pain.
Osteoarthritis and rheumatoid arthritis will also slow healing and recovery time. People with severe arthritis can have no pain in a joint. In fact many times people blame their arthritis pain on tendinosis or tendonitis of the tendons that attach around the joint. Conservative treatment can improve hand and wrist pain; and people will have dramatically less pain in joints that have arthritic changes.
Conclusion
The upper extremity works as a comprehensive unit performing many of the repetitive tasks at home, work, and recreational sports. Injuries to one area of the musculature often indicate that additional damage has been incurred by other muscles.
Many therapeutic exercises can help restore proper strength and endurance to the elbow flexor muscles. Isometric exercises are often the initial treatment exercises. Followed by single plane rubber band exercises for elbow flexion, extension, pronation, and supination movements. Dynamic exercises involving stability ball push-ups can be performed on the wall or floor. The more unstable of the surface the more effort and stabilization is required of all the upper extremity muscles.
Push-ups on a stability ball enhances neuromuscular learning throughout the neck, scapula, shoulder, upper arm, and lower arm muscles. Additional strength exercises can be found on the arm and shoulder strengthening pages.
Our Chandler Chiropractic and Physical Therapy clinic treats patients with a variety of muscle, tendon, joint, and ligament injuries. The clinic provides treatment for runners, tri-athletes, and weekend warriors in addition to common headache, neck, and back patients traditionally seen in Chiropractic, Physical Therapy, Massage Therapy clinics. We work with all ages and abilities of the residents in Phoenix, Tempe, Gilbert, Mesa, and Chandler AZ.